A woman in her forties sits across from me having already tried three antidepressants. Each one raised serotonin the way the textbook promised, and each one left her flat, foggy, and exhausted by two in the afternoon. Her thyroid panel is clean. Her MRI is unremarkable. On paper she is well. She is not well. The story her labs are telling and the story she is living do not match, and the reason is something most psychiatric workups never measure: her brain is running out of fuel.
For sixty years the dominant explanation for depression has been the monoamine hypothesis, the idea that the illness comes down to a shortage of serotonin, norepinephrine, or dopamine. It is a tidy story, and it gave us a generation of useful drugs. It is also incomplete. Roughly a third of patients never respond to SSRIs, and even responders often describe the residue my patient describes: the mood lifts somewhat while the energy, focus, and drive stay broken. A different model is gaining ground, and a study published this year gives it real mechanistic teeth.
What the Cell Metabolism Study Actually Found
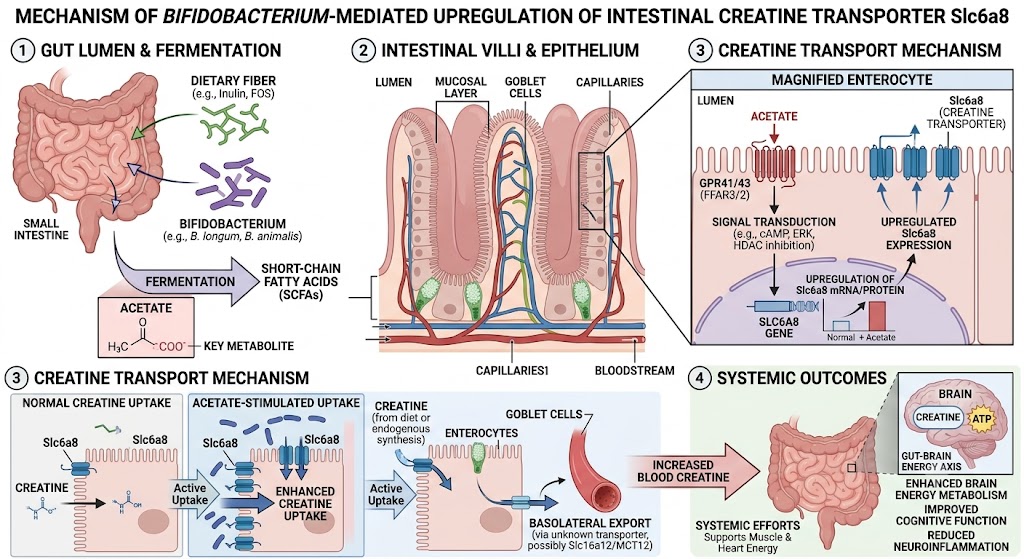
In 2026, Lu and colleagues published work in Cell Metabolism describing a gut-brain energy axis that links a single bacterial genus to depressive symptoms. The finding that should stop every clinician is this: patients with depression had high levels of creatine in their stool but low levels of creatine in their blood and cerebrospinal fluid. The creatine was there. It simply was not getting absorbed.
Creatine is not a bodybuilding curiosity. It is one of the brain's primary energy buffers, the molecule that recharges ATP at the synapse faster than the cell can make it fresh. When brain creatine falls, neurons lose their ability to meet sudden energy demands, and the regions that govern mood and motivation are among the most energy-hungry in the body.
The researchers traced the absorption failure to the gut microbiome. A bacterium called Bifidobacterium pseudolongum was depleted in depressed patients. That bacterium ferments fiber into acetate, a short-chain fatty acid that signals intestinal cells to switch on a creatine transporter named Slc6a8. No bacterium, less acetate. Less acetate, fewer transporters. Fewer transporters, and the creatine you eat passes straight through you instead of reaching your brain. When the team added creatine plus Bifidobacterium to standard antidepressant treatment, plasma creatine rose and depression scores fell against controls. The microbiome was acting as a gatekeeper on the brain's fuel supply.
This is not an isolated signal. Mendelian randomization studies, which use genetics to test causation rather than mere correlation, identify Bifidobacterium as a protective factor against depression, with odds ratios near 0.89. A 2023 trial in JAMA Psychiatry found that a multi-strain probiotic added to antidepressants produced effect sizes of 0.70 for depression and 0.79 for anxiety. The creatine literature is earlier and the quality is still low, but a recent meta-analysis put the pooled effect of creatine supplementation for depression at a standardized mean difference of -0.34. The direction is consistent. The brain that cannot make or buffer energy struggles to hold mood.
Why the Energy Model Explains What Serotonin Cannot
The brain is about two percent of body weight and burns roughly twenty percent of the body's energy at rest. Every thought, every regulated emotion, every act of restraint over a craving is metabolically expensive. When PET imaging shows reduced glucose metabolism in the frontal and limbic circuits of depressed patients, that is not a side effect of low mood. It may be the cause. Mitochondria that cannot keep pace leave neurons unable to sustain the signaling that healthy mood requires.
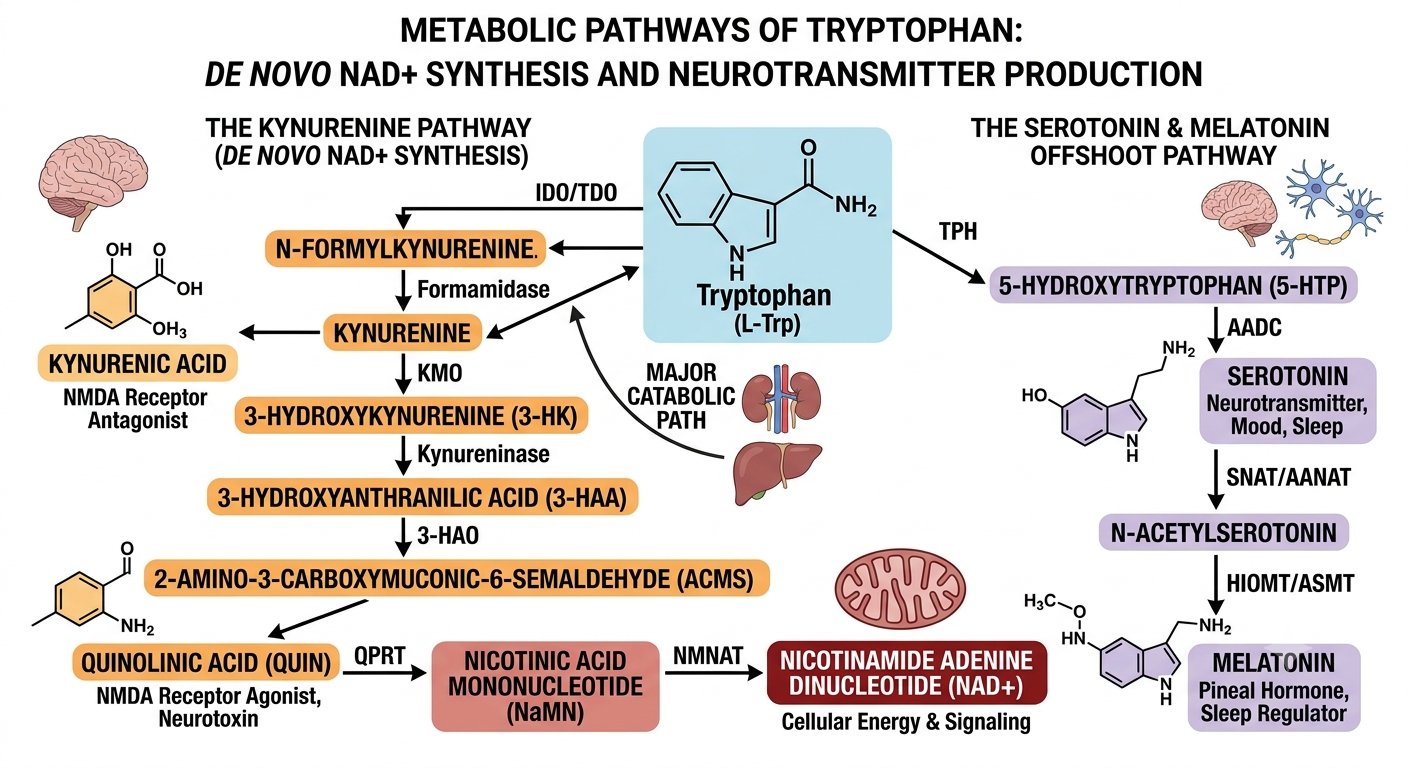
Tryptophan tells the same story from a different angle. Most people associate this amino acid with serotonin, but the brain spends only a sliver of it that way. Under normal conditions roughly ninety-five percent of tryptophan is pulled down the kynurenine pathway, and only about two percent becomes serotonin. The kynurenine pathway is also the body's route to building NAD+ from scratch, the same energy cofactor at the center of this article. So tryptophan sits at a fork: a small branch toward serotonin and melatonin, and a much larger branch that feeds cellular energy. The catch is what happens along that larger branch under inflammation. Pro-inflammatory signals switch on the enzyme IDO, which speeds the conversion of tryptophan into kynurenine and starves the serotonin branch at the same time. Kynurenine can then go two ways: toward kynurenic acid, which quiets NMDA receptors and protects neurons, or toward quinolinic acid, an NMDA agonist that overexcites neurons and damages mitochondria before it is finally converted to NAD+. Inflammation tips this balance toward quinolinic acid. The result is a brain that is at once low on serotonin, low on the neuroprotective metabolite, and carrying a heavier toxic and oxidative load, all from the rerouting of a single amino acid.
Read this way, the symptoms snap into focus. Anhedonia is what a circuit does when it cannot afford to fire. The afternoon crash my patient described is a metabolic ceiling, not a character flaw. And the partial response to SSRIs makes sense too: raising serotonin helps if the machinery downstream has the power to use it, and does little if the cell is energy-starved. This is the gap between a diagnosis and an explanation, and closing it changes what you treat. We covered the broader version of this thinking in our look at how ketamine restores synaptic energy in depression.
This is where measurement changes treatment. We do not guess at where a patient sits on this fork; we test it. By measuring the ratio of kynurenine to tryptophan in blood, we get a direct read on how hard IDO is pulling tryptophan away from serotonin and toward the energy branch, which is one of the clearest objective fingerprints of the inflammation driving a depression. A high ratio tells us the problem is upstream and metabolic, not a simple serotonin deficit, and it points to specific moves: lowering the inflammatory drive on IDO, favoring the kynurenic acid branch over the quinolinic acid branch, and supplying the downstream cofactors that let the pathway end in NAD+ rather than stall at its toxic intermediate. We track the ratio over time the way a cardiologist tracks a lipid panel, adjusting the anti-inflammatory, precursor, and NAD+ components of a protocol until the number moves and the patient's cognition follows. Pairing a mechanism like this with hard biomarkers is the foundation of how we practice, an approach we describe in our look at precision neuromedicine and the data streams that guide it.
How We Restore Brain Energy at The Neurogenesis Project
Naming the problem as energy failure points directly at the fix. At The Neurogenesis Project we approach treatment-resistant depression by rebuilding the brain's metabolic foundation on three fronts, and only after a metabolic workup tells us which front is failing.
The first is mitochondrial function. The same machinery the Cell Metabolism study implicated is what we work to restore, using NAD+ and its precursor NMN to support the electron transport chain, creatine monohydrate to rebuild the phosphocreatine buffer the study found depleted, and N-acetylcysteine to replenish glutathione and protect mitochondria from oxidative stress. Because the new research shows creatine alone often fails to reach the brain, we pair it with a Bifidobacterium-containing probiotic, treating the transporter and the fuel as one problem rather than two.
The second front is the neurotransmitter precursors a stressed brain burns through faster than it can replace. A depleted system cannot manufacture serotonin without tryptophan or dopamine without tyrosine, and methylation stalls without adequate SAM-e. We supply those building blocks directly, through SAM-e, 5-HTP, and the tyrosine and cofactors in our Brain Focus Nootropic Formula. This is where the monoamine model and the energy model meet rather than compete: you give the brain both the raw materials and the power to use them.
The third front is inflammation, which quietly taxes the same mitochondria. Chronic neuroinflammation diverts tryptophan away from serotonin and toward neurotoxic metabolites, and it degrades the energy economy the first two fronts are trying to rebuild. We bring it down with Platinum Turmeric, Relora for the cortisol load that drives it, omega-3 fatty acids for their DHA and EPA, and, for selected patients, mesenchymal stem cell exosomes that carry anti-inflammatory signaling directly into neural tissue. This three-part rebuild is the core of our Intensive Brain Health Program, and it begins with the kind of metabolic and microbiome testing that conventional psychiatry rarely orders.
What This Means If You Have Stopped Responding to Antidepressants
If you have cycled through medications and keep landing back at the same exhaustion, the answer may not be a fourth drug aimed at the same target. The more useful questions are metabolic. Ask whether anyone has measured your inflammatory markers, your micronutrient status, or your gut microbiome. Ask whether your brain has the fuel to use the serotonin a pill is raising. Treatment-resistant is a description of past prescriptions, not a verdict on your biology, and the research is increasingly clear that the biology in question is energetic.
The brain is the asset that produces everything else a person values, and depression is, in part, that asset losing its power supply. The encouraging part of the new science is how addressable that turns out to be. Fuel the cell, fix the transporter, calm the inflammation, and the circuits that govern mood get the energy they were missing. That is a treatable problem, and treating it is the work we do every day.
This article is for educational purposes and is not a substitute for individualized medical care. If you are struggling with depression, talk with a qualified clinician about the options that fit your situation.
References
- Lu CL, Ren J, Lei Y, et al. The gut microbiota alleviates depression by remodeling gut-brain energy metabolism. Cell Metabolism. 2026;38(6):1201–1217.e8. doi:10.1016/j.cmet.2026.03.002
- Chen M, et al. Gut microbiota and major depressive disorder: a bidirectional Mendelian randomization study. Journal of Affective Disorders. 2022;316:187–193.
- Nikolova VL, Cleare AJ, Young AH, Stone JM. Acceptability, tolerability, and estimates of putative treatment effects of probiotics as adjunctive treatment in patients with depression: a randomized clinical trial. JAMA Psychiatry. 2023;80(8):842–847.
- Eckert I, et al. Creatine supplementation for treating symptoms of depression: a systematic review and meta-analysis. British Journal of Nutrition. 2025.